
PRP Study Extended
Dr. Sara Wasserbauer has been asked to enroll more patients in her PRP study. Because of this we will be adding up to 20 additional patients to receive PRP in the coming months (enrollment by June 2023) If you are interested in having this added to your surgery free of cost, call our office to schedule your surgery and reference this email. Here are some recent updates regarding the science of PRP and hair;
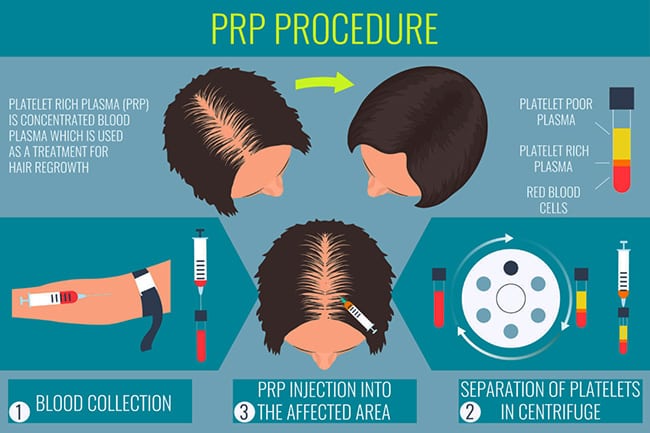
- Hair surgeons use PRP both in their surgeries and as a standalone therapy for hair growth. The current study examines the effects PRP has on wound healing and regrowth post-operatively.
- When PRP is used for hair growth as a standalone treatment, the regimen for initial treatment seems to be 1-3 months for 3-6 treatments, and then 3-6 months thereafter for maintaining the regrowth.
- PRP is NOT a magic hair loss cure. A single treatment does not result in permanent reversal of hair loss.
- PRP volumes, concentrations, and additives are all still actively being debated. For instance, because a patient’s platelet levels vary even within a single day, their platelet concentration and volume available for injection varies, too. This makes tracking results very difficult, and thus additional studies are needed before drawing conclusions about these sorts of variables
Want to be part of the study? Call 925-939-4763
Exclusive PRP/PPP update: Data from our patients
Patients ask all the time: What should be the expected improvement from a PRP treatment? Is there anything else that might work to help my hair?
 Well after combing through 4 years of data - the preliminary results are in! Let me break it down for you:
Well after combing through 4 years of data - the preliminary results are in! Let me break it down for you:
- Our female patients definitely did better with the more frequent (mostly) PRP/PPP treatments. They had a 72% chance of getting an average increase in hair mass of ~25% at 6 months for both the frontal area and the top (crown) areas. More patients will give the statistical analysis more power, but for now we can be confident that these injections have a good chance of helping our female patients – great news!
- Our male patients had a more nuanced picture. Fewer of them chose to inject PRP/PPP alone, but for those that did, the result was an increase in hair mass of about 16% at 6 months. In these patients, the volume injected was lower and the crown area often did not get treated. This is not surprising since 20 ml (the average with PRP/PPP) is about half as much as 10ml so you would expect to cover half the area.
- For those male patients who chose to get PRP/PPP treatments the improvement was about 20% (~4% better than PRP alone) in both the frontal and crown areas at 6 months! Furthermore, the addition of individual adjunctive treatments like finasteride reliably bumped up their results – by about 4-5% of their existing hair mass – with each additional treatment. Here’s what I mean: adding finasteride (Propecia) to the injectable treatments increased the baseline improvement to 24%, adding minoxidil (Rogaine) to that brought it up to about 28%, and adding photobiomodulation treatments (light devices) increased the overall improvement to a whopping 33% in the frontal area! So the “take-home message” is to definitely do as much as you can, all at once and keep it up for 6-12 months because that is what improves hair the most.
 Here are a few other points:
Here are a few other points:
- Currently available Photobiomodulation treatments (i.e. light devices) work best where they can get light through the hair and can independently add as much as 15% improvement. So if you have hair loss to the extent that you can see scalp (but are not yet totally bald), these devices may be worth the investment.
- More frequent treatments (especially for women) and more volume (i.e. more injected area, especially for men) most likely equal more results in most patients. Based on these findings, our office will now double the blood draw volume in order to maximize results for each patient.
- Not all patients’ hair benefits from these treatments, but the data shows it is not likely to be detrimental and may simply help maintain current hair growth levels.
What is old but NEW again in hair treatments?
Off-label, low-dose oral minoxidil. Minoxidil was initially available as an oral and IV blood pressure lowering drug. It was only when the prolific hair-growing effects became obvious that it was made into topical Rogaine. Not many physicians have experience prescribing this medication at low doses for the purposes of treating hair loss, but we do! and it can be remarkable effective and convenient (i.e. no more topical!) for some patients.(2) This is only appropriate for a subset of patients without heart conditions or hypotension (low blood pressure), so call or email to see if it might be right for you!
Off-label, low-dose weekly dutasteride. Dutasteride is usually used to treat an enlarged prostate, but the data shows it is the most effective drug for hair loss available. (3) Significant sexual side effects have prohibited its widespread use, but these effects are dose-dependent, so a low dose that completely avoids sexual side effects may be the answer. A fascinating case study (4) showed that this can have an effect even in older individuals (age 47) and specifically for the crown, so if you are concerned about the back of your head and want to optimize your treatment, this once-weekly medication may be worth a try.
References:
1)1: Kwack MH, Seo CH, Gangadaran P, Ahn BC, Kim MK, Kim JC, Sung YK. Exosomes derived from human dermal papilla cells promote hair growth in cultured humanhair follicles and augment the hair-inductive capacity of cultured dermal papillaspheres. Exp Dermatol. 2019 Jul;28(7):854-857. doi: 10.1111/exd.13927. Epub 2019 Apr 16. PubMed PMID: 30924959.
https://www.ncbi.nlm.nih.gov/pubmed/30924959
2) Pirmez R, Salas-Callo CI. Very low dose oral minoxidil in male androgenetic alopecia: a study with quantitative trichoscopic documentation. J Am AcadDermatol. 2019 Sep 11. pii: S0190-9622(19)32737-9. doi:10.1016/j.jaad.2019.08.084. [Epub ahead of print] PubMed PMID: 31520662.
https://www.ncbi.nlm.nih.gov/pubmed/31520662
3) 1: Olsen EA, Hordinsky M, Whiting D, Stough D, Hobbs S, Ellis ML, Wilson T, Rittmaster RS; Dutasteride Alopecia Research Team. The importance of dual 5 alpha-reductase inhibition in the treatment of male pattern hair loss: results of a randomized placebo-controlled study of dutasteride versus finasteride. J Am Acad Dermatol. 2006 Dec;55(6):1014-23. PubMed PMID: 17110217. https://www.ncbi.nlm.nih.gov/pubmed/171102174) 1: Boyapati A, Sinclair R. Combination therapy with finasteride and low-dosedutasteride in the treatment of androgenetic alopecia. Australas J Dermatol. 2013Feb;54(1):49-51. doi: 10.1111/j.1440-0960.2012.00909.x. Epub 2012 Jun 12. PubMed PMID: 22686691.
https://www.ncbi.nlm.nih.gov/pubmed/22686691
4) 1: Boyapati A, Sinclair R. Combination therapy with finasteride and low-dose dutasteride in the treatment of androgenetic alopecia. Australas J Dermatol. 2013 Feb;54(1):49-51. doi: 10.1111/j.1440-0960.2012.00909.x. Epub 2012 Jun 12. PubMed PMID: 22686691.